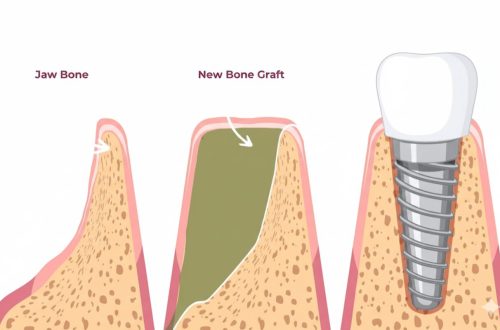
Dental implants have fundamentally transformed modern dentistry, offering the most stable and long-lasting solution for replacing missing teeth. Unlike traditional bridges or removable dentures, a dental implant functions as an artificial tooth root, creating a permanent anchor that integrates directly with the jawbone. This stability is achieved by embedding a fixture—the implant post itself—into the bone, providing an unshakable foundation for the final crown.
For decades, the choice of material for this critical fixture was straightforward: Titanium. This strong, lightweight metal earned its title as the gold standard due to its unmatched strength and exceptional biocompatibility. However, clinical advances have introduced a potent alternative: Zirconia, a high-performance ceramic often referred to as ceramic steel. This material has rapidly gained acceptance, primarily for its aesthetic advantages and metal-free properties.
For the patient, the decision between Titanium vs. Zirconia implants represents a pivotal moment in their treatment plan. The choice is complex, influenced not only by clinical factors like bone density and surgical location but also by patient-specific needs such as aesthetics, systemic health, and budget. This guide provides a comprehensive, objective comparison of these two materials, detailing their design differences, clinical performance, and how each one dictates the long-term reliability and appearance of your smile.
1. The Gold Standard – Titanium Implants
For over four decades, titanium has reigned as the undisputed standard material in implantology. Its unparalleled history of success and specific material properties have established it as the benchmark against which all other implant materials are measured.
1.1. Material Composition & History
The success of titanium is rooted in two core concepts: biocompatibility and osseointegration.
- Composition: Dental implants are typically crafted from commercially pure titanium (cpTi) or a titanium alloy (most commonly Ti-6Al-4V). When exposed to air or body fluids, titanium immediately forms a protective, inert layer of titanium dioxide (TiO2) on its surface.
- Biocompatibility: This TiO2 layer is highly non-reactive, meaning the body does not recognize the implant as a foreign object, minimizing immune response or rejection.
- Decades of Clinical Success: The concept of osseointegration—the direct structural and functional connection between living bone and the surface of a load-bearing implant—was first demonstrated using titanium by Professor Per-Ingvar Brånemark in the 1960s. Since then, billions of titanium implants have been successfully placed worldwide, providing the most robust long-term clinical data in dentistry.
1.2. Key Advantages
The inherent properties of titanium translate directly into several crucial clinical and economic benefits:
- Superior Strength and Durability: Titanium alloys exhibit extremely high tensile strength, elasticity, and fracture resistance. This makes titanium the ideal choice for areas subject to heavy chewing forces, such as the molar and premolar regions (back of the mouth).
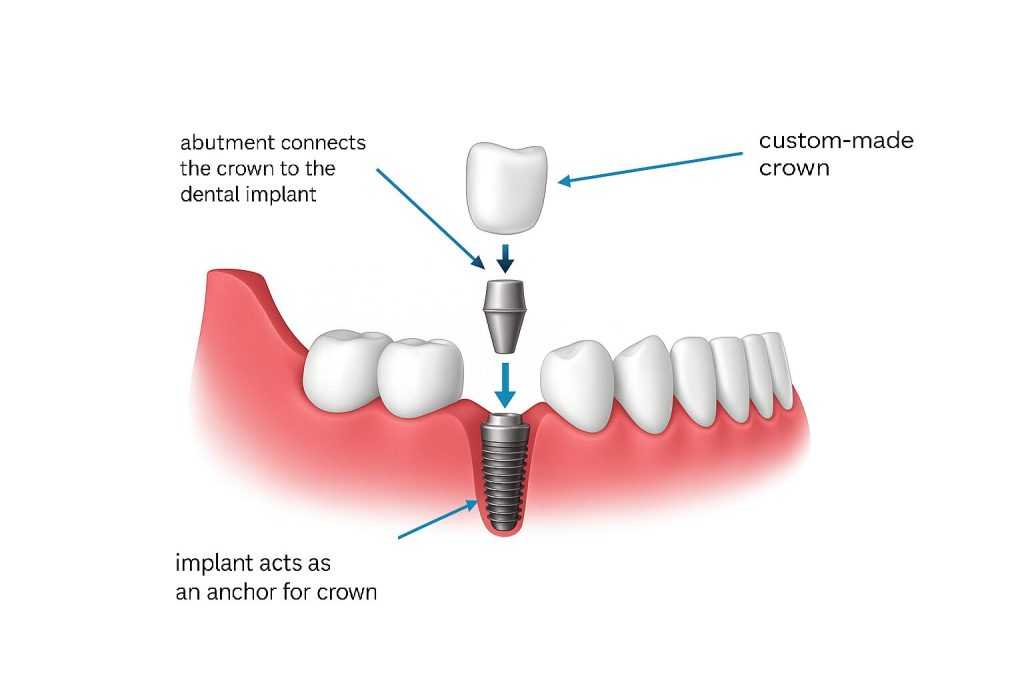
- Two-Piece Design (Modularity): The vast majority of titanium implants utilize a two-piece design , where the implant post (fixture) and the abutment (connector to the crown) are separate components connected by a screw. This modularity allows the dentist to adjust the angle and position of the abutment after the implant has healed, simplifying prosthetic restoration and repair.
- Lower Cost: Due to established manufacturing processes, high availability of the raw material, and competitive market saturation, titanium implants are generally more cost-effective than their ceramic counterparts.
1.3. Disadvantage: The Aesthetic Challenge
Despite its structural superiority, titanium presents a singular, aesthetic drawback, particularly in the highly visible “aesthetic zone” (front teeth).
- The “Grey Shadow” Effect: The naturally dark, metallic color of the titanium implant post can sometimes show through thin gum tissue, especially in patients with a high lip line or very thin gingiva (gums). This creates a visible grey discoloration at the gum line, often referred to as a “tattoo effect”. This aesthetic compromise is the primary reason why alternative materials like zirconia were developed.
2. The Modern Alternative – Zirconia Implants
Emerging as a compelling alternative to titanium, zirconia (zirconium dioxide, ZrO2) addresses the primary aesthetic limitations of metal implants while offering unique biological advantages. While titanium relies on its history, zirconia capitalizes on modern material science.
2.1. Material Composition & Aesthetics
Zirconia is classified as a high-performance ceramic, and its properties have positioned it as a premium option in implantology.
- Composition and Color: Zirconia implants are metal-free and primarily composed of yttria-stabilized tetragonal zirconia polycrystal (Y-TZP). Crucially, the material is naturally white or bone-colored, perfectly mimicking the natural root structure of a tooth.
- Aesthetics: This inherent whiteness is zirconia’s most significant selling point. Unlike titanium, it completely eliminates the risk of the “grey shadow” effect. Even in patients with thin gum tissue, the implant post blends seamlessly with the surrounding anatomy, providing superior long-term aesthetic results.

2.2. Key Advantages
The ceramic nature of zirconia offers biological and aesthetic benefits that titanium cannot match:
- Superior Aesthetics: As mentioned, its white color makes it the ideal choice for aesthetic zones (the front of the mouth), ensuring the final crown and gum line look entirely natural.
- Reduced Plaque Accumulation: Zirconia has an extremely smooth, dense, and non-porous surface. Studies indicate that ceramic surfaces are generally less prone to accumulating bacterial plaque and calculus compared to metal surfaces, potentially leading to a lower risk of peri-implantitis (gum disease around the implant).
- Hypoallergenic: As a metal-free material, zirconia is completely hypoallergenic. For the small subset of patients with documented metal allergies or sensitivities (e.g., to titanium alloys), zirconia offers a safe and proven alternative.
2.3. Disadvantage: Design & Fracture Risk
Despite its advantages, zirconia carries trade-offs that limit its universal application:
- One-Piece Design Rigidity: Historically, most zirconia implants have been manufactured as a one-piece system where the fixture (root) and the abutment (connector) are fused together. This monolithic design enhances strength but severely limits the surgeon’s ability to adjust the angle or placement during surgery, making the prosthetic phase more challenging. While two-piece zirconia systems are now available, they have shorter clinical histories.
- Fracture Risk (Brittleness): Although zirconia is incredibly strong under compression, ceramics are inherently more brittle than metals. This means they are more susceptible to catastrophic fracture under high shear forces or trauma, particularly in areas of high occlusal load.
- Higher Cost: Due to the specialized manufacturing and processing techniques required for ceramics, zirconia implants typically incur a higher cost than titanium implants.
Head-to-Head Comparison (Clinical Factors)
When making the final decision between titanium and zirconia, the focus shifts from individual benefits to direct clinical performance. The comparison hinges on three core factors that determine the long-term success and suitability of the implant for the patient.
3.1. Osseointegration & Biocompatibility
Both materials are considered highly successful in bonding with the jawbone, but their surface dynamics differ slightly:
- Osseointegration Success Rate: Both titanium and zirconia exhibit excellent, clinically proven rates of osseointegration, with both materials showing overall long-term survival rates above 95%. There is currently no substantial clinical evidence suggesting that one material consistently integrates better or faster than the other in a healthy patient.
- Surface Activity: Titanium forms an inert TiO2 layer that promotes bone growth. Zirconia’s ceramic surface is also highly stable and has demonstrated effective cell proliferation (bone-forming cells) in clinical studies.
- Soft Tissue Response (Peri-Implant Health): Zirconia may offer a marginal advantage here. Its smooth surface texture and lower affinity for bacterial plaque can lead to healthier gum tissue attachment and potentially a reduced risk of peri-implantitis over time compared to titanium.
3.2. Strength and Design
The mechanical and structural differences between the two implant types profoundly influence where they can be placed in the mouth:
Titanium (Ti)
- Mechanical Strength: Exhibits extremely high tensile strength and excellent elasticity, making it ideal for withstanding heavy chewing loads.
- Design: Utilizes a Two-Piece (Modular) design, where the implant post and the abutment are separate components. This modularity allows for essential angulation correction and simpler replacement of components.
- Longevity Data: Offers an unmatched clinical history spanning over 40 years, remaining the industry standard with extensive long-term documentation.
Zirconia (ZrO2)
- Mechanical Strength: Possesses high compressive strength but is generally more brittle than titanium. It is susceptible to catastrophic fracture under high shear stress or impact [9].
- Design: Historically favored a One-Piece (Monolithic) design, where the fixture and abutment are a single fused unit. While highly rigid, this limits the surgeon’s prosthetic flexibility and makes angle adjustment challenging.
- Longevity Data: Has a shorter, but rapidly improving clinical history, with documented long-term data spanning approximately 20 years.
3.3. Ideal Placement (The Final Decision)
The patient’s primary need dictates the best material choice:
- When to Choose Titanium (Default Option):
- Posterior Zone (Back Teeth): Recommended for molars and premolars where immense biting forces are exerted, prioritizing durability and superior fracture resistance.
- Complex Cases: Ideal when the implant position is not perfect, as the two-piece design allows the restorative dentist to correct the angle using a customized abutment.
- Budgetary Constraints: Offers a reliable, clinically proven solution at a lower overall cost.
- When to Choose Zirconia (Aesthetic/Specific Needs):
- Aesthetic Zone (Front Teeth): The superior choice for incisors and canines, especially in patients with thin biotypes (thin gums), due to the absence of the metallic “grey shadow”.
- Metal Sensitivity: Mandatory for patients with documented allergies or sensitivities to titanium or its alloys.
- Holistic or Metal-Free Preference: Chosen by patients who prefer a ceramic, non-metal solution for overall body health reasons.
Conclusion
The decision between titanium and zirconia dental implants represents a choice between the proven history of the industry’s gold standard and the advanced aesthetics of modern ceramics. Both materials are clinically superior to older restorative methods and offer high success rates, yet they cater to fundamentally different clinical and patient requirements.
Titanium remains the default choice due to its unrivaled strength, elasticity, and decades of documented clinical performance. Its two-piece modular design offers the surgeon and restorative dentist essential flexibility for angle correction and complex prosthetic work, particularly in the high-stress posterior (back) regions of the mouth. For most general cases, titanium offers the most reliable, cost-effective, and durable foundation available.
Zirconia, while having a shorter clinical history, offers a compelling advantage for specific needs. Its inherent white color makes it the superior material for the highly visible aesthetic zone (front teeth), eliminating the risk of metallic shadowing through thin gum tissue. Furthermore, its smooth, ceramic surface potentially provides a better soft-tissue response, appealing to patients with metal sensitivities or those prioritizing a purely metal-free solution.
Ultimately, the choice is determined by a balanced assessment:
- Prioritize Strength and Modularity: Choose Titanium for molars, complex placements, or when maximal durability is non-negotiable.
- Prioritize Aesthetics and Hypoallergenic Properties: Choose Zirconia for visible front teeth or when biological sensitivities preclude the use of metal.
It is critical that patients consult with a specialist who performs both titanium and zirconia procedures. Only through comprehensive diagnostics and discussion of individual aesthetic goals, budget, and anatomical factors can the optimal material be selected to ensure the long-term success and satisfaction of the implant restoration.